
Supporting women through the physical and emotional experience of perimenopause.
“You are not broken. You are mighty beyond measure. Let’s get your hormones back on your side, so you can emerge from this transition as your most magnificent self!”.
Hi, I'm Louise
I’m a women’s health coach dedicated to helping midlife women feel energised, balanced, and confident again. After experiencing my own struggles with perimenopause, I realised how many women were being told to just “push through” their exhaustion and mood swings. That’s when I decided to create a more compassionate, science-backed approach to support women through this transition.
Through my signature programme, The Peri Protocol, and my workshops, I help women understand what’s really happening in their bodies, manage stress effectively, and make simple lifestyle shifts that restore energy and calm. My mission is to help you feel like yourself again — vibrant, clear, and in control.

YOU DESERVE TO THRIVE DARLING

FREE
From Frazzled to Fabulous
Your perimenopause energy reset guide. In this guide you'll find 5 daily habits to unlock abundant energy. Nutrition, movement, stress reduction and sleep are all important pieces of the energy puzzle. Ditch the brain fog, energy crashes, mood swings, anxiety, insomnia and much more. It's time to feel fabulous!
ARE YOU READY FOR MORE?
Read the blog
Your weekly dose of information, inspiration and practical know-how to transform your life. Nothing is off limits here - nutrition, movement, stress, sleep, intimacy, connection, boundaries. We talk symptoms, science and how you can manage your perimenopause symptoms.
View my services
I am passionate about the role nutrition plays in our physical and mental health and wellbeing. Check out the ways we can work together to help you get back on track and live with more ease.
Connect with me on socials
Where do you like to hang out online? Come and follow me on your favourite platform for inspiration, information and entertainment.
NEW ON THE BLOG...
Ready to build the life of your dreams?
Let's chat
Ready to work with a coach to uplevel your life and business?
Listen to the
Podcast
view my
services
read the
BLOG
Let's chat
Ready to work with a coach to uplevel your life and business?
Let's learn
Learn at your own pace and make quantum leaps.
Student Love Notes
We've helped so many incredible students to find success as Virtual Assistants...

The VA Business Blueprint helped me to go from feeling completely stuck to starting my business and getting my first client!
Ellen, business name

I enrolled in the VA Services Academy feeling completely lost - within 2 weeks I knew exactly what to offer & what to charge.
Ellen, business name

Beginner to Booked Out was a game-changer for me. Anna and her team are incredible and I'm booked out for the next 3 months!
Ellen, business name

The 10 most common perimenopause symptoms (and what actually helps)

7 Signs You Might Be Ready To Consider HRT During Perimenopause
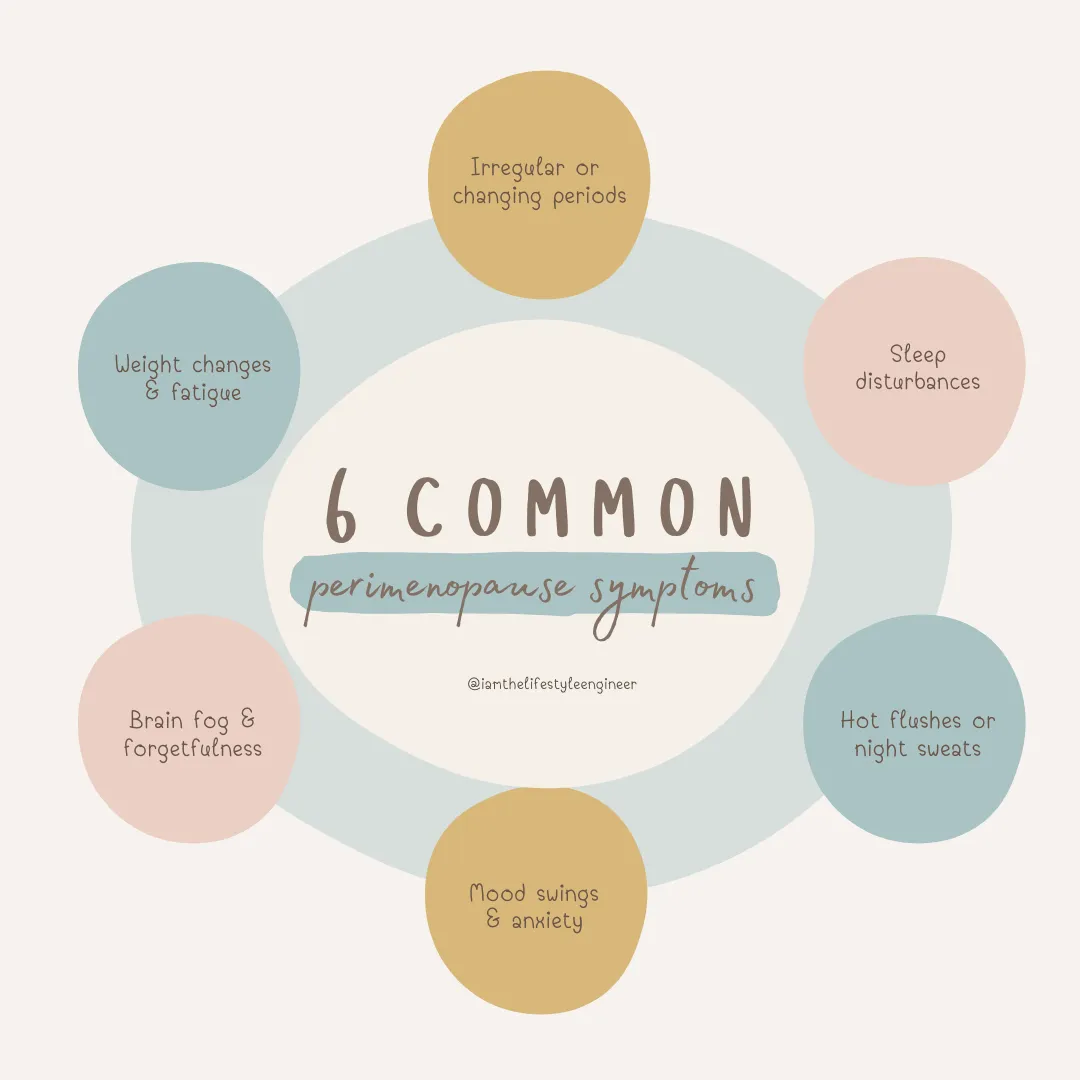
The First 7 Signs of Perimenopause Most Women Miss
New on the blog...

Thinking About Not Taking HRT? Read This
Thinking About Not Taking HRT? Read This
"Do I have to take HRT?"
It's one of the questions I hear most often and it’s a question that I have thought for myself too over the years.
Some women desperately want relief from symptoms but worry about breast cancer. Others simply don't like the idea of taking medication. Some have tried HRT and didn't feel better. Others cannot take it because of their medical history. And many are left wondering whether they should simply "push through" menopause naturally.
There is no single right answer. But not taking HRT is also a health decision. Like every health decision, it has potential consequences.
Those consequences deserve to be understood just as carefully as the potential risks of taking HRT — risks that, as of 2026, are being described very differently than they were even a year ago.
A major shift in how HRT's risks are understood
For over two decades, the use of HRT was linked to cardiovascular disease, breast cancer and probable dementia. That warning traced back to the Women's Health Initiative (WHI) study, released in 2002, which caused hormone therapy use to collapse almost overnight.
Following a lengthy review of scientific literature and expert opinion, it has been accepted that the original WHI findings had been overgeneralized. In that study, the average participant was in her sixties, over a decade past typical menopause onset, and using a formulation that is no longer standard. When the data was reanalyzed by age, women in their forties and fifties who started therapy near menopause showed a different and generally more favourable risk profile.
This doesn't mean HRT is risk-free, and it doesn't erase every question raised by the original research. Individual risk still depends heavily on personal and family history and should be discussed with your doctor. But it does mean the conversation has moved.
Many clinicians and professional bodies now describe HRT started within about 10 years of menopause, or before age 60, as carrying a more favourable balance of benefit to risk than the 2002 warnings implied.
Why does this matter for a woman deciding not to take HRT?
Because some of the fear driving that decision was built on warnings that regulators themselves have now revised. Choosing not to take HRT should be based on your own health history and preferences rather than outdated risk labelling.
Menopause is not simply the end of periods
Menopause is often described as a reproductive milestone.
But biologically, it is much more than that.
For most of a woman's adult life, oestrogen has been influencing almost every organ in her body. Its receptors are found in the brain, heart, blood vessels, bones, muscles, skin, joints, bladder, bowel and immune system. When oestrogen declines, those tissues don't suddenly become diseased but they do begin functioning differently.
Some women notice these changes immediately. Others may not notice them for years. Some changes affect quality of life. Others quietly increase long-term health risks.
Understanding this distinction is important. HRT is not replacing a cosmetic hormone. It is replacing a hormone that has widespread physiological roles throughout the body.
Bones: the clearest example
If there is one area where the evidence is remarkably consistent, it is bone health.
Oestrogen is essential for maintaining the balance between bone formation and bone breakdown. When menopause occurs, bone resorption accelerates. Women can lose up to 20% of their bone density in the years surrounding menopause. This happens whether or not symptoms are severe.
Without intervention, this increases the risk of:
osteoporosis
spinal fractures
hip fractures
loss of independence later in life
Modern hormone therapy remains one of the most effective options for slowing bone loss and reducing fracture risk while it is being used, particularly when started near menopause. This benefit is now being emphasised more strongly, not less.
Does this mean every woman must take HRT? No. Some women choose other medications for osteoporosis. Others rely on resistance training, adequate protein, calcium and vitamin D. But doing nothing should not be mistaken for having no consequences. Bone loss is largely silent until the first fracture.
The heart changes too
Before menopause, women generally develop cardiovascular disease later than men. Researchers believe oestrogen contributes to this protection through favourable effects on blood vessels, cholesterol metabolism and vascular function.
As oestrogen declines, cardiovascular risk gradually rises. Weight distribution changes. Blood pressure often increases. Insulin resistance becomes more common. LDL cholesterol tends to rise while HDL often falls.
HRT is still not prescribed as a stand-alone strategy purely to prevent heart disease. But the evidence base here has strengthened: when started within about 10 years of menopause or before age 60, cardiovascular effects appear neutral or potentially favourable, compared with a less favourable, and possibly harmful picture when started much later, in women who already have established atherosclerosis. This "timing hypothesis" acknowledges that early initiation is associated with a more favourable cardiovascular profile.
The important point is this: whether or not you take HRT, menopause represents a turning point for cardiovascular health. Ignoring blood pressure, cholesterol, muscle mass and physical activity becomes increasingly costly.
Your muscles are changing—even if the scales don't show it
One of the least discussed effects of menopause is muscle.
From midlife onwards, women naturally lose muscle mass and strength. Lower oestrogen contributes to this process. Many women notice that tasks which once felt effortless become harder. Recovery after exercise takes longer, balance changes, and falls become more common.
Muscle is not just about appearance. It influences blood sugar regulation, metabolism, bone strength, mobility and independence.
HRT may help preserve lean body mass in some women, but resistance training, adequate protein intake and regular movement remain essential regardless of hormone use. This is why exercise becomes more important after menopause.
The brain: what we know and what we don't
Many women describe feeling as though their brain has changed. They struggle to find words, forget names, lose concentration, and feel mentally slower.
These experiences are real. Oestrogen receptors exist throughout the brain, and fluctuating hormones can affect sleep, attention and memory.
Whether HRT prevents long-term cognitive decline or dementia remains genuinely uncertain. The original "probable dementia" warning was based on data from women in their late sixties and seventies, an age group well past the window in which HRT is typically started. This generalisation should not be applied to younger women. That doesn't mean HRT protects the brain. Research on HRT and long-term dementia risk in women who start therapy near menopause is still ongoing.
What we can say with more confidence is that untreated hot flushes, disrupted sleep and chronic stress can impair cognitive performance and quality of life. For many women, improving those symptoms indirectly improves how their brain functions day to day.
The tissues nobody talks about
One consequence of low oestrogen receives surprisingly little public attention.
The tissues of the vagina, vulva, bladder and urethra are oestrogen dependent. Without treatment they often become thinner, drier and less elastic. Over time this can contribute to:
painful sex
recurrent urinary tract infections
urinary urgency
bladder irritation
reduced sexual function
Unlike hot flushes, these symptoms often become progressively worse rather than resolving naturally.
The good news is that local vaginal oestrogen is highly effective and can often be used even by women who cannot use systemic HRT, depending on their individual medical circumstances. This local, low-dose treatment has long been considered to carry a different, generally more favourable safety profile than systemic therapy.
The emotional cost matters too
When we discuss menopause, we often focus on disease. But health is more than avoiding disease, it is also about living well.
Poor sleep, persistent hot flushes, joint pain, anxiety, loss of confidence, reduced libido, and exhaustion.
These affect relationships, careers, parenting and overall wellbeing. Sometimes women minimise these symptoms because they don't seem life-threatening. Yet quality of life is a legitimate reason to seek treatment. Living well matters.
Choosing not to take HRT is still an active decision
There are completely valid reasons not to take HRT.
Some women have medical contraindications. Some have previously experienced breast cancer. Some simply decide that the risks, however small, are not acceptable for them. That is a reasonable and informed choice, and it's one that should be made with your doctor, weighing your personal and family history..
But if you choose not to use HRT, it becomes even more important to actively protect the systems that oestrogen once supported. That means prioritising:
progressive resistance training
daily physical activity
adequate protein
sufficient calcium and vitamin D where needed
cardiovascular risk assessment
blood pressure and cholesterol monitoring
maintaining muscle mass
protecting sleep
limiting smoking and excessive alcohol
discussing bone density testing with your doctor when appropriate
treating vaginal symptoms early rather than assuming they are inevitable
Menopause is not a time to become less proactive. it is a time to become more intentional.
The real question
When deciding if you want to use HRT, it is important to think about your personal health history, symptoms, family history and goals. You are looking at the best strategy to protect your health over the next 30 to 40 years.
For many women, that strategy includes HRT. For others, it does not. Neither choice is automatically right. Whether you choose HRT or not, there are many ways that you can support your body and brain during perimenopause, many of which HRT cannot provide either way.
You might be interested to read my article “The 10 Most Common Perimenopause Symptoms: And What Actually Helps”.
The best decision is an informed one, built on current evidence. Because menopause is not simply about surviving hot flushes. It is about building the healthiest possible second half of your life.
This article reflects hormone therapy research as of early 2026. It is general information, not personal medical advice. Talk to your doctor about what's right for your history and circumstances.

